Changing Approach to Health Care
The Home Care Medical Revolution

Source:Chien-Tong Wang
Cloistered in their hospitals, many Taiwanese physicians have not realized that patients’ homes can turn into prisons harmful to their health. That is now changing as a home care revolution takes shape, but plenty of obstacles remain.
Views
The Home Care Medical Revolution
By Yi-ting LinFrom CommonWealth Magazine (vol. 619 )
A 53-year-old man, let’s call him Chen Jun-ming, has not left the confines of his apartment in the 15 years since he suffered a stroke and was discharged from the hospital. During that time, he has not been to see a doctor or done any rehabilitation.
The old apartment building he lives in Taipei only has stairs, and he’s in no condition to climb them as a result of the stroke. His family members are scared to carry him up and down the stairs, fearing that a fall could have disastrous consequences.
Complicating matters is that his relatives live busy lives and don’t know how to get outside help.
“At the time of discharge, the doctor said rehabilitation was necessary, but I was really busy with work at the time,” says one of Chen’s older brothers, with whom Chen lives, helplessly. “I don’t know how to take care of him.”
Whenever Chen Jun-ming gets a cold or feels pain, his family members buy drugs. Because Chen has not sought treatment or done any rehabilitation over a long period of time, his limbs have atrophied, and he even needs the help of others to sit down.
His nearly 90-year-old mother and 66-year-old older brother are nearing points where they no longer have the physical strength to carry the load, and their poor posture in taking care of their loved one has taken a toll on their backs.
Filling a Major Gap in Care
Now, however, an integrated home health care revolution is taking shape that promises to improve the lives of people who have disabilities or are incapacitated.
“If coming here is inconvenient, we’ll send our medical team to your home,” says Taipei City Hospital Superintendent Huang Sheng-jean, who has been nicknamed the “medical reformer.”
Led by the local ward chief, a medical team from the Zhongxing Branch of Taipei City Hospital armed with medical devices now visits Chen Jun-ming every two to three weeks. The branch hospital’s superintendent, Liu Chih-kuang, treats Chen and prescribes medicine, and physical therapist Tu Zhi-ming designs rehabilitation moves suitable for the home environment and teaches family members how to help.
The involvement of the home care team has improved Chen Jun-ming’s condition. He can sit up on the edge of his bed by himself, and where he once feared seeing people, he is now gradually regaining the use of his hands and welcoming visits, exchanging high-fives and other greetings with the medical team.
Patients are not the only beneficiaries of the integrated home health care program. Because medical teams now visit people’s homes, family members no longer have to constantly take time off from work to take their elders to see a doctor or spend a lot of time and effort driving around or shuttling between hospital clinics.
The Integrated Home Health Care Project also covers cradle to grave care and shows concern for the family members of patients.
One example is the treatment of Lin Yu-feng (another pseudonym), who died at the age of 95 of terminal cancer in the comfort of her home in mid-March 2017.
Though Lin’s family was saddened by her passing, they showed no signs of panic or anxiety. Lin had received regular visits from the director of the Family Medicine Division at the Zhongxing Branch of Taipei City Hospital, Sun Wen-jung, who provided palliative care, taking her off chemotherapy and medicines that only increased her pain. Family members knew that if there was a change in Lin’s condition, they could call a 24-hour hotline to seek assistance, which ultimately helped them to prepare themselves mentally for Lin’s death.
“I would get worried when Mom’s health took a turn for the worse, but Director Sun told us not to worry, that with a phone call we could get help from somebody at any time of the day or night. That helped us relax,” says Lin’s daughter-in-law, who took care of the elderly family matriarch.
That hotline access was a change for the better, explains the daughter-in-law, who previously rushed to the emergency room every time Lin’s condition changed. “Taking her to the hospital was exhausting for both her and me,” the daughter-in-law remembers.
Medical professionals involved in home care treat more than the patient’s symptoms; they also focus on the patient’s overall lifestyle and the family.

Home Care that Prevents Suffering
“At the heart of medicine is caring. Its aim is to prevent the suffering of patients, families and medical teams,” Taipei City Hospital’s Huang stresses in discussing the philosophy behind the home care concept. “It even strives to prevent the suffering of society as a whole.”
Huang’s argument in defense of the approach is backed by solid evidence. According to research done in the United States, patients who received integrated home care saw their emergency room visits plummet by 29 percent and their hospitalization rate fall by 11 percent within the first year of being treated at home, saving considerable medical expenses and resources.
In Taiwan, “statistics show the 10 percent of people who use the national health insurance system the most consume about 60 percent of the resources. If we can take good care of that 10 percent, we could use resources more efficiently,” says Lee Yue-Chune, a professor in National Yang-Ming University’s Institute of Health and Welfare Policy. Lee notes that many of the 10 percent are elderly people with chronic diseases who lack mobility or are incapacitated.
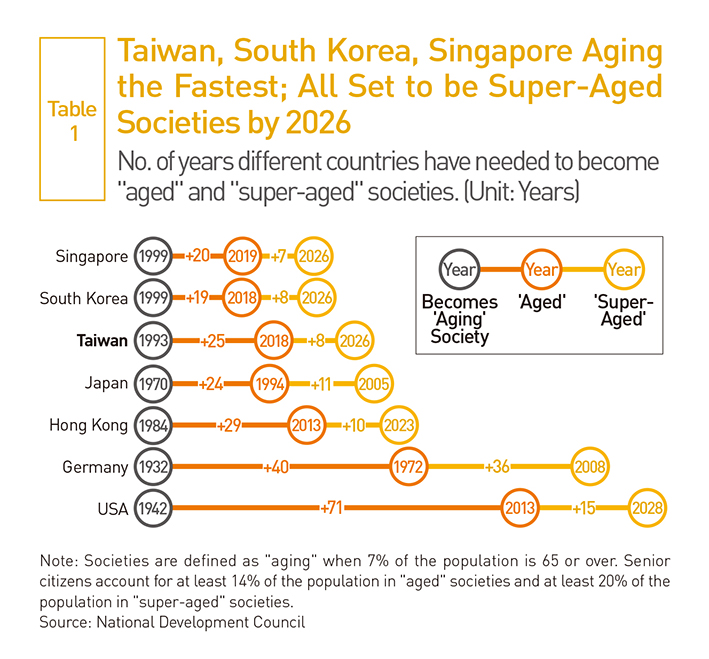
Taiwan has lagged behind the U.S., Europe and Japan in developing home care, but because it is aging faster than almost any country in the world, it needs to pick up the pace. In February 2017, the number of people in Taiwan 65 and over reached 13.3 percent of the total population and next year will surpass 14 percent – the threshold for an “aged” society – according to the latest Ministry of the Interior statistics. (Table 1)
2017 has also seen Taiwan become a society in which senior citizens outnumber children and young teenagers. The convergence of a low birth rate and the trend toward aging pushed Taiwan’s Aging Index above 100 for the first time, to 100.2, in February, meaning that the number of people 65 and over now exceeds the number of people younger than 15 years old. (Table 2)
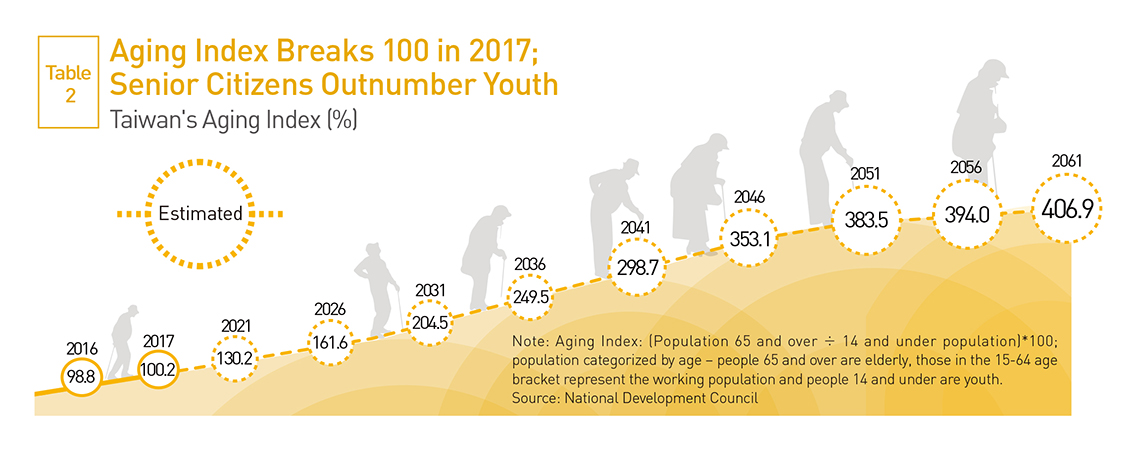
The Aging Index – the ratio of the elderly population to the youth population – was only 72 in Taiwan as recently as 2011, statistics show, reflecting the torrid pace at which the country’s population is getting older.
Estimates indicate that the elderly will account for 20 percent of Taiwan’s population by 2026, reaching the threshold for a “super-aged” society that Japan has already hit.
In the not-too-distant future, Taiwan will emerge as the oldest country in the world. Based on statistics released by the United Nations Population Division, the countries with the three highest median ages in 2015 were Japan (46.5), Germany (46.2) and Italy (46.1).
Taiwan’s median age of 40.6 in 2016 seems a long way away.
But based on current aging trends, Taiwan will have a median age of 55.6 by 2050, according to Ministry of the Interior projections. That would be higher than any country in the U.N. projections, including the top two finishers, South Korea (53.9) and Japan (53.3).
At present, Taiwan has 760,000 people with disabilities or who are incapacitated, a number expected to rise to 1.2 million by 2030. Only by changing the existing system of centralized, specialized health care can the country hope to make good use of the national health insurance system’s resources.
In such an environment, Taipei City Hospital’s Huang has fired the first salvo of reform. Instead of trying to upgrade the city’s hospital system into “medical centers,” which would entitle it to greater resources, Huang is encouraging the more than 600 physicians and more than 1,000 medical staff at the seven hospitals in the Taipei City Hospital system to get out of their ivory tower.
As of February 2017, nearly 100 doctors in the Taipei City Hospital system were taking part in the initiative and providing care to 1,768 people, nearly a quarter of all patients receiving integrated home care in Taiwan.
New Realizations
But promoting the integrated home care program has not been without its challenges, among the biggest of which is that medical workers have been unwilling to leave their comfort zone.
When Huang first pushed the concept in Taipei City Hospital, he faced a severe backlash.
“Medical teams wondered ‘why do we have to go into the field?’” he recalls. “They looked at the project with disdain, then rebuffed it and then passively resisted it.”
The director of the Urology Department of the Taipei City Hospital’s Zhongxing Branch, Ko Ming-chung, understood how his colleagues felt. Having practiced medicine for 26 years, he was used to spending most of his time in the hospital’s outpatient clinic or operating room.
 Huang Sheng-jean (right) has convinced nearly 100 Taipei City Hospital doctors to see patients at their homes. One of them, Sun Wen-jung (left), has persisted with the program despite being treated as a fraudster by families and not allowed in or having to make visits in typhoons.
Huang Sheng-jean (right) has convinced nearly 100 Taipei City Hospital doctors to see patients at their homes. One of them, Sun Wen-jung (left), has persisted with the program despite being treated as a fraudster by families and not allowed in or having to make visits in typhoons.
“Going out wasn’t convenient,” he says, describing how he felt about the integrated home care program.
But after Ko made the effort to leave his ivory tower, he felt ashamed. “When I arrived at his home, I told the patient ‘I’m sorry. I didn’t realize you had to go through so much to get treatment.’”
Only by going to people’s homes did Ko realize how difficult it was for one of his outpatients, polio-suffering 66-year-old “Ah Kuo,” to visit the hospital many times over the years to see his doctor for 10 minutes.
Ah Kuo’s legs had atrophied, and not only did he have to enlist the help of a sympathetic taxi driver to carry him down the stairs, he also had to apply for help from an NGO to accompany him once he got to the hospital. But when waiting times at the hospital were long, social workers became antsy because of other commitments they had.
“They would not always accommodate you. There were times they made things hard when they were with you,” says Ah Kuo helplessly. He was even stopped by Dr. Ko when he tried to cut in line at Ko’s outpatient clinic because of Ko’s insistence on seeing patients in the order in which they registered.
“Over the past 30 to 40 years, medicine has made progress. So why have doctor-patient relationships gotten worse? Because doctors have not rediscovered the basic importance of ‘people.’ If a group of organ specialists focus on treating organ-related diseases, how can people-to-people relations get better?” wonders Huang.
“This initiative is giving doctors the chance to reflect on their practices.”
But change cannot solely depend on doctors taking stock of themselves. The system also has to be ameliorated. The current lack of incentives for offering home care is the major reason medical workers are reluctant to invest time and effort in the program.
To get doctors to leave their comfort zone, the National Health Insurance Administration (NHIA) has begun to mull improving internal processes. According to Lin Shu-fan, a senior executive officer with the NHIA’s Medical Affairs Division, the rates at which the NHIA reimburses hospitals for home care have been increased, and the agency plans to continue to streamline administrative procedures that have come under criticism.
Getting Local Clinics on Board
An even bigger challenge, however, is to encourage local clinics to get involved in the home care revolution.
“Neighborhood clinics are like local ‘gods of the land.’ Land gods manage life and manage death,” Taipei City Hospital’s Huang says.
Taiwan’s more than 10,000 clinics reach into all corners of the country, and should be the main practitioners of home care because of their penetration of local communities and ability to care for people in their neighborhoods.
But as of the end of 2016, only 596 clinics were participating in the integrated home care project, only 5.6 percent of the total. In Japan, that figure is closer to 20 percent, nearly four times the rate of participation seen in Taiwan.
Part of the problem is that doctors run their own clinics and tend to go it alone, while home care usually requires cooperation with other medical units. The need to organize three-phase teams, offer 24-hour consultation hotlines and handle cumbersome administrative tasks and paperwork has deterred clinics from getting involved.
By giving guidance to smaller clinics, including sharing its home care methods and assisting with administrative procedures, Taipei City Hospital has persuaded 55 clinics to participate.
“If we have a question, including on regulations or registration procedures, we can raise them at any time, and the system superintendent [Huang Sheng-jean] will answer them promptly,” says Zheng Wei-li, who has his own clinic in Wanhua and joined the home care program at an early stage because of Taipei City Hospital’s support.
Outside of Taipei, the move to join the home care trend has only just begun.
Though the NHIA started last year to include “home care” in the evaluation criteria of its “Family Physician Program” to encourage greater participation, only 28 percent of Taiwan’s 414 community medical groups were involved in integrated home care as of the end of last year, meaning that plenty of work remains to be done.
Out of the Loop: Long-term Care
One other major challenge facing this budding home care revolution is the longstanding lack of integration between medical care and social welfare. “In the past, the 10-year long-term care plan was not connected to national health insurance. Long-term care was long-term care, and health care was health care,” National Yang-Ming University’s Lee says.
That has led to fragmented care – medical workers offered one set of diagnoses and recommendations while long-term caregivers gave their own prescriptions for care.
 Taipei Mayor Ko Wen-je (right), a longtime physician, now goes on home care visits with Taipei City Hospital teams to get a feel for people’s needs.
Taipei Mayor Ko Wen-je (right), a longtime physician, now goes on home care visits with Taipei City Hospital teams to get a feel for people’s needs.
Of the 17 types of services that are covered in Taiwan’s “Long-term Care 2.0” program – which was proposed in July 2016 and began on a trial basis in November – two address this problem: “home care” and “discharge preparation.” The two services make it possible for people who are incapacitated to get cohesive care, and they fill in much needed pieces in the community-care puzzle.
But even the most basic information integration issues have not been resolved. The NHIA’s Lin acknowledges that a system integrating information on home care was launched at the beginning of this year, but while medical workers can use it, it cannot be accessed by long-term care units.
With Taiwan’s society aging rapidly, the home care revolution is spreading. But the ultimate challenge for the country is how its national health insurance and medical systems, facing a mountain of intertwined problems from the past and present, can create a path that allows the revolution to press forward and deliver high-quality, reliable care? It’s a question that will challenge the wisdom of the medical and political communities.
Translated from the Chinese by Luke Sabatier

Views

Subscribe to CWE Newsletter (every Thursday)
Stay abreast of what's happening in Taiwan with our weekly digest.