Time to Change Taiwan’s Medical System
No More ‘Kidney Dialysis Island’

Source:Justin Wu
Taiwan has the dubious distinction of having more end-stage renal disease per capita than anywhere in the world, leading to heavy use of kidney dialysis. That will only change if the health insurance system and prevailing attitudes undergo overhauls.
Views
No More ‘Kidney Dialysis Island’
By Yi-ting Linweb only
Every Tuesday, Thursday and Saturday, a taxi driver waits outside the office of Chen Wen-yu to pick him up, not for regular business appointments but for a 20-minute ride to a kidney dialysis center.
“I’ve been doing this for seven years. I originally was able to ride a bike [to the center], but my stamina has been on the decline, and there were a few times when I nearly passed out on the road. So now I take a taxi,” says Chen, not his real name to protect his identity.
He always takes a bag with him filled with food, water, bandages, and tourniquets to make it through the 4-hour dialysis process.
The 64-year-old Chen began his regular dialysis regimen when he was 57. At the time, his doctor told him he needed dialysis because his diabetes was getting worse and damaging his kidney functions. For the father of three children still in school, it was a huge shock that dealt a stinging blow to both him and his family.
“It was hard for me to accept. My oldest son even told me he didn’t want to continue his studies,” Chen recalls. But as the head of the household, Chen “wanted to stay alive, so I started doing it. At first, the dialysis ordeal would push me to tears – it was really tough – but now I’m more used to it.”
He cannot rely on urine to flush unwanted toxins from his body, instead depending on a four-hour kidney dialysis three times a week to survive. The process he is undergoing – hemodialysis – involves drawing blood from his arm and then filtering it through a manmade membrane, or dialyzer, to get rid of waste before sending the clean blood back into the body.
“I only realized how important kidneys are after I got sick,” says Chen, lying on his back, staring up at the ceiling with his sleeves rolled up.
Dotting his left arm are patches of purple, the ravages of long-term dialysis. His frequent hospital trips have taken a toll on his work, the orders received by his factory having fallen by half.
The Catalyst of ‘Kidney Dialysis Island’
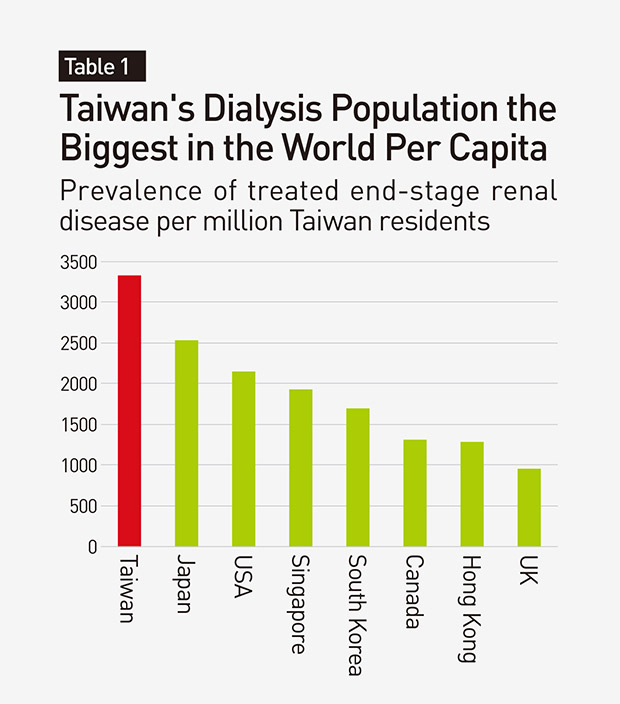
Taiwan has nearly 85,000 kidney dialysis patients who face similar ordeals.
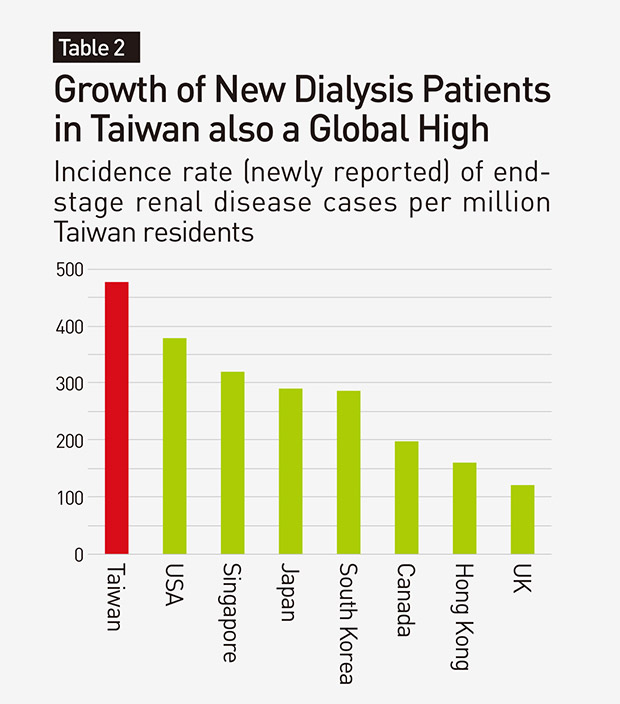
That translates to 3,317 people per 1 million population suffering from end-stage renal disease (ESRD), commonly recognized as the most in the world. Also, 476 new cases of ESRD are diagnosed in Taiwan per year, another global high on a per capita basis. These trends have earned Taiwan the infamous title of “Kidney Dialysis Island.”
Many factors account for the growing number of dialysis patients. An aging population and an increase in chronic diseases such as diabetes and hypertension have contributed to the rise in ESRD cases, and the abuse of Chinese herbal medicine and painkillers accelerate kidney damage.
But another, perhaps less obvious culprit, is Taiwan’s national health insurance system, a key catalyst of “Kidney Dialysis Island.”
“If the health insurance system continues on its present course, Taiwan will remain known as ‘Kidney Dialysis Island,’” says Taiwan Society of Nephrology President Lu Kuo-cheng. “Health insurance has its pluses but also its minuses.”
On the plus side, the health insurance system has accelerated the development of Taiwan’s dialysis technology.
“In the past, kidney dialysis was not well-developed, and [ESRD] patients faced certain death. Nephrologists were known as the “corpse collection brigade. Nobody wanted to do the job,” Lu says.
“But after the health insurance system was put in place, nephrology departments became important,” he says, observing that doctors were more willing to get involved in kidney care and medical technology advanced.
At present, the 5-year survival rate for dialysis patients in Taiwan is nearly 60 percent, second only to Japan, which has led to the ongoing growth in dialysis patient numbers.
The health insurance system has also made it possible for patients to survive without bankrupting their families, especially with reimbursements for kidney dialysis in Taiwan more generous than in other countries.
 Image: Justin Wu
Image: Justin Wu
Neglecting the Importance of Prevention
In a book he co-authored on Taiwan’s national health insurance system, Control Yuan member Huang Huang-hsiung found that from its inception in 1996 the system has covered more than 10 items related to severe kidney disease, including epoetin injections and drug costs, and unlike in South Korea or Hong Kong, there are no co-payments.
But that blanket coverage has had a downside, according to Huang’s report, which concluded that the “completely free kidney dialysis system” has been one of the factors behind the surge in kidney dialysis patients and medical expenditures.
The number of dialysis patients has risen from 23,000 in 1996 to 85,000 last year, and overall spending on dialysis has risen from NT$11.3 billion to NT$48.3 billion over that time. That’s a roughly four-fold increase in both categories over the health insurance system’s existence.
Lee Po-chang, the director-general of the National Health Insurance Administration (NHIA), says that if one adds the amount spent on the hospitalization of kidney dialysis patients for complications, total spending on dialysis patients per year comes to NT$60 billion, nearly 10 percent of the system’s total expenditures.
“We have to confront the kidney dialysis problem. If we don’t, no matter how wealthy the country is or even if we institute second, third, or fourth-generation insurance programs [to increase receipts], the system will collapse,” Lee warns.
The problem gained greater urgency last year when a study published in the prestigious medical journal The Lancet sent shockwaves across Taiwan.
The study compared the Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories between 1990 and 2015. Taiwan ranked 44th overall with an average score of 78, but its score of 50 for the treatment of chronic kidney disease was its lowest for any disease other than leukemia and ranked 84th in the world, behind such countries as Tanzania, Burkina Faso, Uzbekistan, Gabon and China. To a country that prides itself on its national health insurance system and medical technology, the finding was truly alarming and sparked a debate in medical and political circles.
An in-depth look at the problem by CommonWealth Magazine has uncovered three major changes that need to be made to the health insurance system and general approaches and attitudes if Taiwan is to break away from its fate as “Kidney Dialysis Island.”
Change No. 1: New Approach to Chronic Disease
“The problem isn’t that the quality of kidney dialysis in Taiwan is bad. It’s that not enough is done on prevention, so patients who need dialysis keep popping up,” says Lin Hsien-ho, an associate professor in National Taiwan University’s Department of Public Health.
“We’ve actually talked about prevention for more than 10 years, but Taiwan’s efforts in this area are still inadequate.”
The vice superintendent of Kaohsiung Medical University Hospital, Hwang Shang-jyh, says the findings of the Lancet study may have been the alarm that was needed.
“The study was a real slap in the face for us, but it also opened our eyes. We had thought that putting so much effort into the ‘back-end’ [dialysis treatment] would be meaningful to patients. But based on the global trend, we need to put more resources and thought into the ‘front-end,’ into prevention,” says Hwang, a nephrologist by trade.
But prevention can be difficult when there’s a general lack of awareness among the general public.
There are an estimated 2 million people in Taiwan with chronic kidney disease, but only 3.5 percent of them know they have a problem. In addition, many people are unaware that diabetes and hypertension are linked to the need for kidney dialysis.
“I thought it was just diabetes. I didn’t feel like anything was wrong even if I didn’t take medicine,” says dialysis patient Chen. But when doctors told him a few years later that his condition had worsened and he needed dialysis, Chen felt regret.
“If my doctors could have warned me earlier, maybe I would have treated my condition more aggressively and controlled my diet better. That may have only put off the need for dialysis by 3-5 years, but that still would have been great,” he says.
Although the Ministry of Health and Welfare has launched a series of prevention campaigns over the years, including the promotion of a “diabetes shared care network” and a “chronic kidney disease care program,” their impact has been limited. Of the new kidney dialysis patients in Taiwan every year, hypertension accounts for 15 percent of the cases and diabetes 45 percent, the latter factor up 11 percentage points from 10 years ago.
The lack of cooperation between the Health Promotion Administration, the National Health Insurance Administration, and hospital departments remains a serious problem.
The director of Taipei Veterans General Hospital’s Center for Geriatrics and Gerontology, Chen Liang-kung, contends that medical departments are too narrowly defined in Taiwan’s medical system, with different departments caring separately for the different conditions a person might have.
That does not work well for older patients, who tend to have several related ailments that all affect the quality of care for chronic diseases, Chen says.
Kaohsiung Medical University Hospital’s Hwang agrees, arguing that to combat the “Kidney Dialysis Island” stigma, different medical departments must work together.
“Heart, liver, brain, kidney, diabetes – doctors from all of these departments should care for patients together,” he says. In fact, Hwang is currently engaged in getting all of the professionals in his hospital, from doctors to nutritionists and health educators, to provide integrated care across medical specialties.
For example, health educators in different departments should have knowledge of more than one discipline, Hwang says. “They shouldn’t just consider their own specialty. They need to focus on the whole picture.”
An even more fundamental approach would be to promote health education and good habits from when people are young, such as the need to pay attention to the ingestion of carbohydrates, sugary drinks, and proteins and the importance of regular exercise.
“Without a sense of responsibility, there’s no point in talking about anything else,” says Lu, the Taiwan Society of Nephrology president.
He suggests that the national health insurance system could even take a page from compulsory automobile liability insurance and charge higher premiums to those who act in ways that harm their health, such as excessive eating or drinking. That would increase the responsibility and obligation of every individual, and let them know that the system “cannot provide unlimited free treatment.”
Lu acknowledged, however, the difficulty of putting such an approach in place, noting that it would trigger a backlash and that government agencies have elections to worry about.
“I proposed this 10 years ago at the Control Yuan, but legislators and the Ministry of Justice haven’t raised the idea. Behind closed doors, everybody says it’s a good idea, but once the doors open, they forget about it.”
Change No. 2: Promote Kidney Transplants
Though kidney dialysis is widespread, the global medical community actual favors transplants when a patient’s kidneys no longer function normally.
Though transplants have limitations and the surgery carries inherent risks, survival rates are relatively high and patients do not have to return to the hospital on a regular basis.
“I’ve been doing kidney transplants for 38 years, and I’ve seen countless numbers of wives getting divorces from their husbands because of the toll of long-term dialysis,” says the NHIA’s Lee, who is also a surgeon specializing in kidney transplants. “But if there’s a chance to get a transplant, it can change families’ fates.”
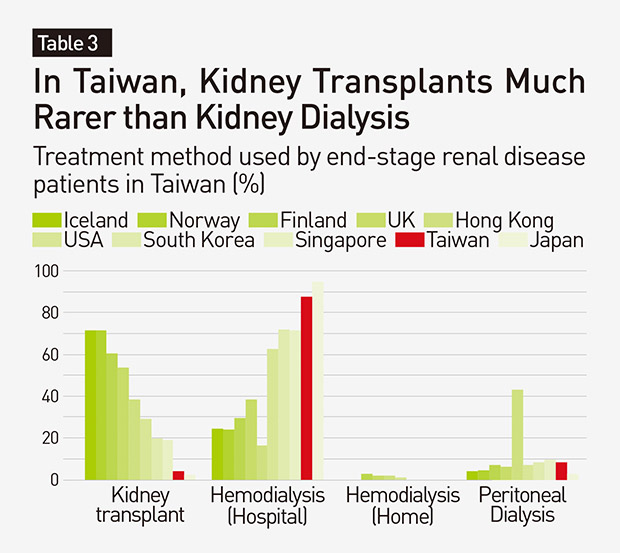
The odds of getting that chance in Taiwan, however, are extremely long. Only 300 people in Taiwan have successful kidney transplants a year, a mere 4 percent of ESRD patients, compared with 50 percent in England and Scandinavian countries.
Wang Chu-yu, a 53-year-old kidney transplant patient waited 11 years before getting a new kidney, yet “I still consider myself lucky. The average wait is about 33 years,” he says with a touch of irony. At present, 7,000 people are on the waiting list in Taiwan.
One problem is the lack of organ donors, in part driven by the cultural tradition of keeping the body whole at death or the misconception among men that donating a kidney can lead to impotence. In contrast, the legal framework in many countries actually encourages organ donation.
Another issue is the impact the national health insurance system has had on medical behavior.
“The reimbursement system tacitly encourages dialysis and does not encourage kidney transplants,” says Wen Chi-pang, a professor with the Institute of Population Health Sciences at the National Health Research Institutes.
The health insurance system reimburses dialysis procedures based on the “number” performed, which makes a difference to hospital income and physicians’ salaries. Based on the reimbursement rate of 4,000 points [hospital services are calculated in points and then converted to Taiwan dollars according to several factors] per dialysis, if a hospital has 50 patients, and each one has dialysis done three times a week, that’s NT$30 million per year in revenue for the hospital, Wen says.
“Even though there are costs, there is also plenty of profit, which is why so many kidney dialysis centers have sprung up,” Wen says. “If transplants become the main option, that NT$30 million per year in revenue disappears.”
According to NHIA statistics, the number of beds for dialysis patients rose five-fold to 18,434 in 2016 from when the national health insurance system was launched in 1996. But Wen stresses that “the problem is not doctors; it’s the health insurance system.”
The NHIA’s Lee says the reimbursement for kidney transplants was increased last year to encourage nephrologists to promote “kidney transplants as a substitute for kidney dialysis.” Under the plan, if a patient has their kidney successfully replaced, a hospital can receive a bonus of 50,000 points. But the plan’s impact has been limited, with only one such case recorded in 2017.
For the policy to spur change, another step is needed, Lee argues. “The Ministry of Health and Welfare is mulling whether to tie reimbursements of kidney dialysis and kidney transplants together. Otherwise, nephrology departments will continue to see kidney transplants as the business of surgical departments and something that is unrelated to them.”
The idea is expected to be put on the agenda at the coordination meeting for the national health insurance system’s global budget in 2019.
 Image: Justin Wu
Image: Justin Wu
Change No. 3: Offer End-of-life Choices
As populations age, organ failure becomes increasingly common, turning decisions on whether or not to save patients into value judgments.
In Taiwan, the idea of keeping people alive to the bitter end still remains prevalent both among doctors and the general public. More than 3,400 people here have their first kidney dialysis after the age of 75, up 85 percent from 10 years earlier. That rate of growth far surpasses that of other age groups.
“You have to spend so many days of your last stage of life in a kidney dialysis room next to a dialysis machine,” says Chu Hsien-kuang, the deputy head of the Taiwan Healthcare Reform Foundation. “Clearly listing one’s end-of-life wishes or holding a family meeting can lead to a better use of resources and allow the patient to pass on with dignity and bid farewell to family members.”
Beyond the family’s sentiment, doctors’ attitudes and actions are also critical to making such decisions. “Some doctors think they are like gods and can’t fathom the idea of giving up. So they keep fighting and fighting,” Kaohsiung Medical University Hospital’s Hwang says.
But in fact doctors can play a more constructive role.
“Medical professionals represent the biggest hurdle to overcome. If a team of doctors would just say the word, it would open families’ minds and help them make a decision on the kind of life they want,” observes Kung Lan-fang, a CKD (chronic kidney disease) educator at Kaohsiung Medical University Hospital, based on her many years working with families.
 Image: CW
Image: CW
Offering “choices” is not only the responsibility of hospitals but also the retirement homes where many dialysis patients reside.
Mrs. Liu, an 87-year-old resident of one such home has dementia and heart disease and has been undergoing dialysis for nearly 16 years. In recent years, she has lived at ZhiShan Senior Home in Taipei because her complicated condition made it impossible for her family to take care of her. Three days a week, her daughters-in-law take turns accompanying her to the hospital for her dialysis treatment.
“Can I not go?” Mrs. Liu has asked them, tired of the many years of pain caused by her ailments and the side effects of the dialysis. There are also times when she has to be rushed to the hospital because of re-occurring infections or emergencies, leaving everyone exhausted.
But things changed last year when with the help of the nursing home they gradually gained an understanding of the concept of “hospice care,” learning, for example, what would happen if the dialysis was discontinued, what kinds of drugs could alleviate the resulting discomfort and how end-of-life issues should be faced.
“In Taiwan, many patients and families have never thought about the option of hospice care. We get involved at an early stage and help them prepare,” says Chou Chyn-chen, the director of Zhishan Senior Home.
In the end, Mrs. Liu’s family decided not to continue with her dialysis. Two weeks later, she passed away in the nursing home with her children and grandchildren at her side.
“We felt very sad about this, but the decision didn’t cause any pain or anger,” says one of Mrs. Liu’s sons. “Mom no longer has to endure the pain, and she smiled and interacted with us far more in those last few days than she had for many years.”
Taiwan has voiced its intention to shake off its reputation of being a “Kidney Dialysis Island” for more than 10 years. But for real change to occur and reduce the suffering of people across Taiwan, doctors from different medical specialties, government agencies and the public need to cast aside their ingrained biases toward each other and work together in pursuit of the goal.
Translated from the Chinese article by Luke Sabatier
Additional Reading
♦ Taiwan’s ER Crisis
♦ Psychosomatic Disorders: Taiwan’s New Health Killer
♦ WHO: Healthcare Costs are Pushing Millions into Extreme Poverty, This Outrage must End

Views

Subscribe to CWE Newsletter (every Thursday)
Stay abreast of what's happening in Taiwan with our weekly digest.





